FREEDOM with honesty, justice, and courage..
COMPASSION with dignity, humour, and tolerance..
KNOWLEDGE with effort, perseverance and sharing..
LOVE with peace and harmony towards all
LIFE ON EARTH.
A science-based international free press humanitarian organization...
created in 1972.. human4us2.blogspot.com...
“Our ultimate goal here is to obtain structural information on antibodies and their binding sites, and use that to guide SARS-CoV-2 vaccine design, just as our lab has done with influenza and HIV,” says the study’s co-first author Nicholas Wu, PhD, a postdoctoral research associate in the Wilson lab.
The new study centers on an anti-SARS-CoV antibody called CR3022 that was originally isolated in 2006 by the pharmaceutical company Crucell Holland B.V. in the Netherlands. A report from Chinese scientists earlier this year indicated that CR3022 cross-reacts against SARS-CoV-2. Wilson’s team used their structural mapping expertise to determine how the antibody binds to SARS-CoV-2.
A key finding is that the antibody’s binding site is highly similar between the two coronaviruses—differing by just four protein building blocks called amino acids. That high degree of similarity implies that the site has an important function that would be lost if it mutated significantly.
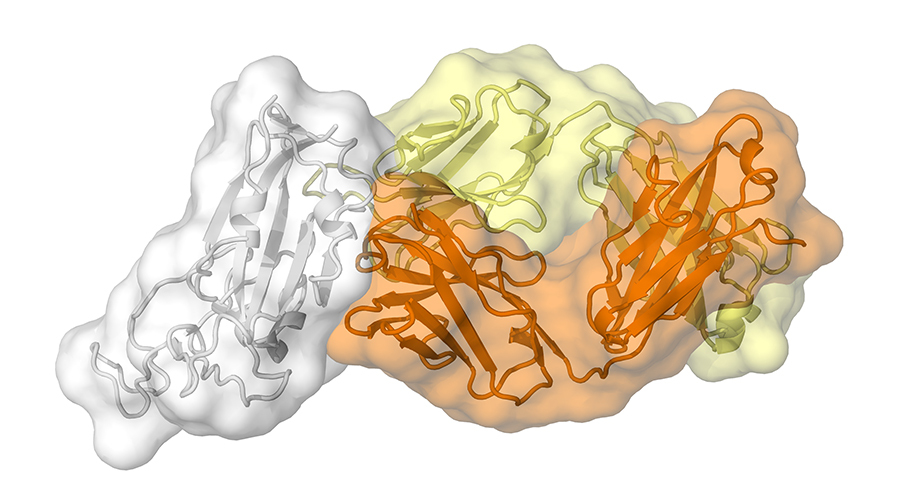
An antibody called CR3022, produced by a patient in response to the coronavirus that causes SARS, also binds to the new coronavirus that causes COVID-19. (Image courtesy of Meng Yuan and Nicholas Wu of the Wilson lab.)
Clues to COVID-19 coronavirus’s vulnerability emerge from an antibody against SARS
A Scripps Research study reveals a likely site of vulnerability on the SARS-CoV-2 virus.
April 03, 2020
LA JOLLA, CA — An antibody recovered from a survivor of the SARS epidemic in the early 2000s has revealed a potential vulnerability of the new coronavirus at the root of COVID-19, according to a study from scientists at Scripps Research.
The study, published today in Science, is the first to map a human antibody’s interaction with the new coronavirus at near-atomic-scale resolution. Although the antibody was produced in response to an infection of SARS (severe acute respiratory syndrome), which is caused by the SARS-CoV virus, it cross-reacts with the new coronavirus, SARS-CoV-2.
The structural mapping revealed a nearly identical site on both coronaviruses to which the antibody binds, suggesting a functionally important and vulnerable site for this family of coronaviruses.
“The knowledge of conserved sites like this can aid in structure-based design of vaccines and therapeutics against SARS-CoV-2, and these would also protect against other coronaviruses—including those that may emerge in the future,” says the study’s senior author Ian Wilson, DPhil, Hansen Professor of Structural Biology and Chair of the Department of Integrative Structural and Computational Biology at Scripps Research.
SARS-CoV, which causes SARS, originated in horseshoe bats, but jumped to humans in South China in 2002, eventually infecting more than 8,000 people and killing almost 800 before it was quelled by lockdowns, quarantines and other measures.
SARS-CoV-2, a closely related coronavirus that causes COVID-19, first emerged in the Chinese city of Wuhan in late 2019. Much more infectious than its viral cousin, it has led to a pandemic, causing far more cases of illness and fatalities than SARS. The development of a vaccine or even an effective treatment could significantly ameliorate the crisis.
The Wilson lab is known for its pioneering structural studies of antibodies bound to viruses including HIV and influenza. These studies have been used to inform designs of vaccines and antibody drugs, as well as other therapeutics. Along with hundreds of other labs around the world, Wilson’s team is now focused on SARS-CoV-2.
“Our ultimate goal here is to obtain structural information on antibodies and their binding sites, and use that to guide SARS-CoV-2 vaccine design, just as our lab has done with influenza and HIV,” says the study’s co-first author Nicholas Wu, PhD, a postdoctoral research associate in the Wilson lab.
The new study centers on an anti-SARS-CoV antibody called CR3022 that was originally isolated in 2006 by the pharmaceutical company Crucell Holland B.V. in the Netherlands. A report from Chinese scientists earlier this year indicated that CR3022 cross-reacts against SARS-CoV-2. Wilson’s team used their structural mapping expertise to determine how the antibody binds to SARS-CoV-2.
A key finding is that the antibody’s binding site is highly similar between the two coronaviruses—differing by just four protein building blocks called amino-acids. That high degree of similarity implies that the site has an important function that would be lost if it mutated significantly.
Yet, the site’s function remains mysterious. The Scripps Research analysis found that the antibody binding site is relatively remote from the part of the virus that grabs hold of cell-surface protein receptors in preparation for penetrating cells in our lungs. That suggests that, at least for SARS-CoV, CR3022 neutralizes the virus’s ability to infect cells in some indirect way.
Adding to the mystery is the finding that the antibody binding site on these viruses is not normally accessible to antibodies.
“We found that this region is usually hidden inside the virus, and only exposed when that part of the virus changes its structure, as it would in natural infection,” says co-first author Meng Yuan, PhD, also a research associate in the Wilson lab.
Despite the slightness of difference between the two coronaviruses, the antibody binds much less tightly to SARS-CoV-2 than it does to the SARS virus, and cannot neutralize SARS-CoV-2 in lab dish tests as it does SARS-CoV.
Still, the findings suggest that the binding site for this antibody on SARS-CoV-2 is a site of vulnerability, and that antibodies binding it more tightly would plausibly succeed in neutralizing the virus. Such neutralizing antibodies, if developed into therapies, could be used to treat COVID-19 patients and to provide temporary protection from the virus to uninfected individuals, for example healthcare workers.
The fact that this binding site is highly conserved between SARS-CoV and SARS-CoV-2 also hints that there may be antibodies, still to be discovered, that can effectively neutralize both viruses—and perhaps in the same way, can neutralize future emergent coronaviruses before they can cause pandemics.
Labs at Scripps Research and throughout the world are currently seeking antibodies, via blood donations, from people who have recovered from COVID-19 for further studies along these lines.
Hello Gentle People: There are laboratories around the world in search of a cure for the Covid-19 epidemic but so far, and after checking six potential cures, I have narrowed it down to Four with above-average promise. Three therapies with promise against SARS-CoV-2. 1. Convalescent plasma therapy. 2. Pluristem therapy. 3. CRISPR editing. 4. ACE2 The first uses cells from the human placenta and the second uses blood plasma from patients who have recovered from Covid-19. Both these methods are being tested with some success reported against Covid-19. The third method listed is CRISPR, a method for genetically changing the RNA or DNA of a human or animal cell. Research hints that CRISPR might be a useful tool to destroy viruses. How that will work is a good question and I am going to do some research to find out. CRISPR does hold promise for the future but how long into the future remains anybody's guess. The fourth ACE2, is showing good results in laboratories around the world. Chinese researchers have now used cryogenic electron microscopy (cryo-EM) to study the structure of the ACE2 when it is bound to one of its typical ligands, the amino acid transporter B0AT1 and also how the COVID-19 RBD may bind to the ACE2-B0AT1 complex. These structures have previously not been identified and could aid in producing antivirals or a vaccine that can block coronavirus infection by targeting ACE2.
----------------------------------------------------
Antiviral drugs still under study.
1. Ivermectin
2. Colchicine
3. Remdesiver
---------------------------------------------------------
New information:
The sars-coV-2 virus attacks not only the lungs but every organ in the body. Early use of a Thrombin inhibitor to prevent thromboembolism, (blood clotting) is recommended. A direct thrombin inhibitor is VE-1902, a member of a novel class of precision oral anticoagulants (PROACS) that combine effective anticoagulation with reduced bleeding.
-------------------------------------------------
The Chinese are providing a massive amount of information for scientific research. Go to:https://www.nature.com/articles/s41586-020-2223-y_reference.pdf
The 670-kilometre, $6.2 billion pipeline is buying off the Native band councils of Vancouver, one by one, however, money for nursing homes across Canada is not available.
In Canada, today, our Federal and Provincial governments claim they do not have enough money for the production of protective gear to help fend off the Corona-virus or to pay for extra doctors and nurses to work in nursing homes. Consequently, hundreds of alone and abandoned vulnerable older people across Canada are dying alone and without help.
The truly unjust part of this story is that there is plenty of money to spend on an unwanted and dangerous gas pipeline through First Nations territory in Vancouver. For the first time in their lives, some natives are working and benefitting from the work provided by the Gas pipeline industry, but they are working by cutting down trees and preparing the way for the passage of a dangerous fossil fuel pipe-line that will continue producing CO2 and creating industrial pollution for years into the future. Natives and non- natives alike could easily be working saving forests and planting trees or working in thousands of Greenhouse gardens within reserves or on farms across the country if provided with the same amount of federal money the gas industry is receiving. A gas industry backed by our present prime minister who is paying with our tax dollars. If the Covid 19 SARS epidemic teaches us anything, it is that we do not have enough years to reverse or stop global warming. Do you remember global warming? Why do you think viruses are having such an easy time destroying our lives? A warmer climate breeds viruses. For imperial Dollars and the blessing of the Prime Minister of Canada, First Nations band councils are bought and paid for by the Gas industry and are going against the history and culture of their own people while helping a dangerous and cruel industry pollute the Earth!
Wednesday, April 15, 2020
What Scientists Know About Immunity to the Novel Coronavirus
Though COVID-19 likely makes recovered patients immune, experts aren’t sure how long protection lasts
Can you become immune to SARS-CoV-2? (Radoslav Zilinsky / Getty Images)
Resolving the COVID-19 pandemic quickly hinges on a crucial factor: how well a person’s immune system remembers SARS-CoV-2, the virus behind the disease, after an infection has resolved and the patient is back in good health.
This phenomenon, called immune memory, helps our bodies avoid reinfection by a bug we’ve had before and influences the potency of life-saving treatments and vaccines. By starving pathogens of hosts to infect, immune individuals cut off the chain of transmission, bolstering the health of the entire population.
Scientists don’t yet have definitive answers about SARS-CoV-2 immunity. For now, people who have had the disease appear unlikely to get it again, at least within the bounds of the current outbreak. Small, early studies in animals suggest immune molecules may stick around for weeks (at least) after an initial exposure. Because researchers have only known about the virus for a few months, however, they can’t yet confidently forecast how long immune defenses against SARS-CoV-2 will last.
“We are so early in this disease right now,” says C. Brandon Ogbunu, a computational epidemiologist at Brown University. “In many respects, we have no idea, and we won’t until we get a longitudinal look.”
A memorable infection
When a pathogen breaches the body’s barriers, the immune system will churn out a variety of immune molecules to fight it off. One subset of these molecules, called antibodies, recognizes specific features of the bug in question and mounts repeated attacks until the invader is purged from the body. (Antibodies can also be a way for clinicians to tell if a patient has been recently infected with a given pathogen, even when the microbe itself can no longer be detected.)
Though the army of antibodies dwindles after a disease has resolved, the immune system can whip up a new batch if it sees the same pathogen again, often quashing the new infection before it has the opportunity to cause severe symptoms. Vaccines safely simulate this process by exposing the body to a harmless version or piece of a germ, teaching the immune system to identify the invader without the need to endure a potentially grueling disease.
From the immune system’s perspective, some pathogens are unforgettable. One brush with the viruses that cause chickenpox or polio, for instance, is usually enough to protect a person for life. Other microbes, however, leave less of an impression, and researchers still aren’t entirely sure why. This applies to the four coronaviruses known to cause a subset of common cold cases, says Rachel Graham, an epidemiologist and coronavirus expert at the University of North Carolina at Chapel Hill. Immunity against these viruses seems to wane in a matter of months or a couple of years, which is why people get colds so frequently.
Because SARS-CoV-2 was only discovered recently, scientists don’t yet know how the human immune system will treat this new virus. Reports have surfaced in recent weeks of people who have tested positive for the virus after apparently recovering from COVID-19, fueling some suspicion that their first exposure wasn’t enough to protect them from a second bout of disease. Most experts don’t think these test results represent reinfections. Rather, the virus may have never left the patients’ bodies, temporarily dipping below detectable levels and allowing symptoms to abate before surging upward again. Tests are also imperfect, and can incorrectly indicate the virus’ presence or absence at different points.
Because the COVID-19 outbreak is still underway, “if you’ve already had this strain and you’re re-exposed, you would likely be protected,” says Taia Wang, an immunologist and virologist at Stanford University and the Chan Zuckerberg Biohub. Even antibodies against the most forgettable coronaviruses tend to stick around for at least that long.
COVID-19 packs a stronger punch than the common cold, so antibodies capable of fending off this new coronavirus may have a shot at lingering longer. Broadly speaking, the more severe the disease, the more resources the body will dedicate to memorizing that pathogen’s features, and the stronger and longer lasting the immune response will be, says Allison Roder, a virologist at New York University. Previous studies have shown that people who survived SARS, another coronavirus disease that resulted in a 2003 epidemic, still have antibodies against the pathogen in their bloodyears after recovery. But this trend is not a sure thing, and scientists don’t know yet whether SARS-CoV-2 will fall in line.
Earlier this month, a team of researchers posted a study (which has yet to be published in a peer-reviewed journal) describing two rhesus macaques that could not be reinfected with SARS-CoV-2 several weeks after recovering from mild bouts of COVID-19. The authors chalked the protection up to the antibodies they found in the monkeys’ bodies, apparently produced in response to the virus—a result that appears to echo the detection of comparable molecules in human COVID-19 patients.
But the mere presence of antibodies doesn’t guarantee protection, Wang says. Reinfections with common cold coronaviruses can still happen in patients who carry antibodies against them. And a bevy of other factors, including a person’s age and genetics, can drastically alter the course of an immune response.
An evolving virus?
Complicating matters further is the biology of SARS-CoV-2 itself. Viruses aren’t technically alive: While they contain genetic instructions to make more of themselves, they lack the molecular tools to execute the steps, and must hijack living cells to complete the replication process for them.
After these pathogens infect cells, their genomes often duplicate sloppily, leading to frequent mutations that persist in the new copies. Most of these changes are inconsequential, or evolutionary dead ends. Occasionally, however, mutations will alter a viral strain so substantially that the immune system can no longer recognize it, sparking an outbreak—even in populations that have seen a previous version of the virus before. Viruses in the influenza family are the poster children for these drastic transformations, which is part of why scientists create a new flu vaccine every year.
When flu viruses copy their genomes, they often make mistakes. These errors can change the way their proteins look to the immune system, helping the viruses evade detection. (Rebecca Senft, Science in the News)
Some viruses have another immunity-thwarting trick as well: If a person is infected with two different strains of the flu at the same time, those viruses can swap genetic material with each other, generating a new hybrid strain that doesn’t look like either of its precursors, allowing it to skirt the body’s defenses.
Researchers don’t yet know how quickly similar changes could occur in SARS-CoV-2. Unlike flu viruses, coronaviruses can proofread their genomes as they copy them, correcting mistakes along the way. That feature reduces their mutation rate, and might make them “less of a moving target” for the immune system, says Scott Kenney, an animal coronavirus expert at Ohio State University. But coronaviruses still frequently trade segments of their genetic code with each other, leaving the potential for immune evasion wide open.
So far, SARS-CoV-2 also doesn’t appear to be undergoing any extreme mutations as it sweeps across the globe. That may be because it’s already hit on such a successful strategy, and doesn’t yet need to change its tactic. “Right now, it’s seeing a completely naive population” that’s never been exposed to the virus before, Graham says. The virus “doesn’t seem to be responding to any kind of pressure,” she adds.
Should SARS-CoV-2 get a second infectious wind, it may not come for some time. Even fast-mutating influenza strains can take years to reenter populations. And if or when that day comes, future COVID-19 outbreaks could be milder. Sometimes viral success means treading gently with the host, says Catherine Freije, a virologist at Harvard University.
“Viruses that causes severe disease actually tend to die out faster because a host that’s feeling ill can’t spread it as well.” In those cases, she says, sometimes, “the outbreak just sort of fizzles out.”
But we can’t rule out the possibility that SARS-CoV-2 could change in a way that bumps up its virulence instead, Kenney says. To steel the population for what’s ahead, sometimes, he adds, “We just have to be the ultimate pessimist when it comes to this type of outbreak.”
Protection without disease
Although much about COVID-19 remains unknown, researchers are racing through vaccine development to boost the world’s collective immunity—something that would stem the spread of the virus through the human population.
“Vaccine development is going to be critical to controlling this outbreak,” says Wang. That’s especially true if SARS-CoV-2 returns for an encore act. “If it’s an ever-present pathogen, we’ll certainly need vaccines to be part of our arsenal.”
Researchers have managed to concoct partially effective vaccines to combat other coronavirus infections in animals, such as pigs. In these creatures, immunity lasts “at least several months, possibly longer,” says Qiuhong Wang, a coronavirus expert at Ohio State University. (Because many of the subjects are livestock, they often don’t live long enough for researchers to test them further.) These vaccines may be reason for hope, she says, pointing out that “humans are animals, too.”
Two flu viruses can sometimes infect the same host cell. When they spill their contents into the cell, their genetic material can recombine, generating new hybrid viruses that are mixtures of their precursors. (Rebecca Senft, Science in the News)
Several research teams are designing human vaccines that trigger the production of antibodies that attack SARS-CoV-2’s spike protein—the molecular key the virus uses to unlock and enter human cells. Because the spike protein is crucial for viral infection, it makes an excellent target for a vaccine, says Benhur Lee, a virologist at the Icahn School of Medicine at Mount Sinai. But Lee also points out that the spike protein, like other parts of the virus, is capable of mutating—something that could compromise the ability of a vaccinated individual to ward off the virus.
If mutation regularly occurs to that extent, scientists may need to frequently reformulate COVID-19 vaccines, like they do with pathogens in the flu family, Wang says. “We’d be starting over to some degree if there is a new outbreak.”
However, Wang cautions that it’s too soon to tell whether that will be the case. As research worldwide proceeds at breakneck speed, scientists may instead be able to brew up a universal vaccine that’s active against multiple forms of SARS-CoV-2.
But vaccines, which require rigorous testing and retesting to ensure efficacy and safety, take a long time to develop—typically more than a year, Qiuhong Wang says. In the meantime, researchers are turning their attention to treatments that could save those who have already been infected.
Some solutions will inevitably require antiviral drugs that tackle active SARS-CoV-2 infections after they’ve already begun, usually by interfering with the virus’ infection cycle.
But another approach, based on a time-tested technique, also taps into the immune response: transferring blood plasma—and the disease-repelling antibodies it contains—from recovered patients into infected ones. Though new to the current pandemic, the treatment has been deployed in various forms since the 1890s, and saw modest success during outbreaks of SARS in 2003 and Ebola in 2014. Ongoing trials in New York are now recruiting carefully screened, healthy volunteers who no longer have symptoms or detectable virus in their bodies to donate plasma. Importantly, this doesn’t diminish donors’ own resistance to SARS-CoV-2, since their immune systems have already learned to manufacture more antibodies.
Antibodies degrade over time, and won’t protect the people who receive these transfusions forever. The plasma treatments also can’t teach their recipients’ immune systems to make new antibodies after the first batch disappears. But this stopgap measure could ease the burden on health care workers and buy time for some of the outbreak’s most vulnerable victims.
Even as the pandemic evolves, researchers are already looking ahead. Just as the response to this outbreak was informed by its predecessors, so too will COVID-19 teach us about what’s to come, Qiuhong Wang says. The entry of other coronavirus strains into our species “is inevitable.”
“We don’t know when or where that will happen,” she says. But hopefully by the time the next pandemic comes around, the world will be more ready.
/https://public-media.si-cdn.com/filer/e1/40/e1406e36-48fe-4f32-b5de-f635a661af13/gettyimages-1212213050.jpg)



