FREEDOM with honesty, justice, and courage..
COMPASSION with dignity, humour, and tolerance..
KNOWLEDGE with effort, perseverance and sharing..
LOVE with peace and harmony towards all
LIFE ON EARTH.
A science-based international free press humanitarian organization...
created in 1972.. human4us2.blogspot.com...
Genome-wide CRISPR screens for SARS-CoV-2, HCoV-229E, and HCoV-OC43 host factors
•
Screens correctly identified divergent entry factors for the three coronaviruses
•
Cholesterol and phosphatidylinositol pathways are shared host dependency factors
•
Pharmacological inhibition of host factors reduces coronavirus replication
Summary
The Coronaviridae are a family of viruses that cause disease in humans ranging from mild respiratory infection to potentially lethal acute respiratory distress syndrome. Finding host factors common to multiple coronaviruses could facilitate the development of therapies to combat current and future coronavirus pandemics. Here, we conducted genome-wide CRISPR screens in cells infected by SARS-CoV-2 as well as two seasonally circulating common cold coronaviruses, OC43 and 229E. This approach correctly identified the distinct viral entry factors ACE2 (for SARS-CoV-2), aminopeptidase N (for 229E), and glycosaminoglycans (for OC43). Additionally, we identified phosphatidylinositol phosphate biosynthesis and cholesterol homeostasis as critical host pathways supporting infection by all three coronaviruses. By contrast, the lysosomal protein TMEM106B appeared unique to SARS-CoV-2 infection. Pharmacological inhibition of phosphatidylinositol kinases and cholesterol homeostasis reduced replication of all three coronaviruses. These findings offer important insights for the understanding of the coronavirus life cycle and the development of host-directed therapies.
The Coronaviridae family includes seven known human pathogens for which there are no approved vaccines and only limited therapeutic options. The seasonally circulating human coronaviruses (HCoV) OC43, HKU1, 229E, and NL63 cause mild, common cold-like respiratory infections in humans (
van der Hoek, 2007). However, three highly pathogenic coronaviruses emerged in the last two decades, highlighting the pandemic potential of this viral family (
Zaki et al., 2012). Infection with severe acute respiratory syndrome coronavirus 1 (SARS-CoV-1) and Middle East respiratory syndrome coronavirus (MERS-CoV) can lead to acute respiratory distress syndrome and death, with fatality rates between 10%–40% (
Petersen et al., 2020). SARS-CoV-2, though less deadly, is far more transmissible than SARS-CoV-1 and MERS-CoV and has been responsible for over 50 million cases and 1.2 million deaths globally as of November 2020 (
Petersen et al., 2020). Because of the severity of their impact on global health, it is critical to understand how SARS-CoV-2 and other coronaviruses hijack the host cell machinery during infection and apply this knowledge to develop new therapeutic strategies.
Coronaviruses are enveloped, positive-sense single-stranded RNA viruses with a genome length of approximately 30 kb. Upon receptor binding and membrane fusion, the viral RNA is released into the cytoplasm, where it is translated to produce viral proteins. Subsequently, the viral replication/transcription complexes form on double-membrane vesicles and generate genome copies. These are then packaged into new virions via a budding process, through which they acquire the viral envelope, and the resulting virions are released from infected cells (
Fung and Liu, 2019). During these steps, specific cellular proteins are hijacked and play crucial roles in the viral life cycle. For example, the angiotensin-converting enzyme 2 (ACE2) is exploited as the viral entry receptor for NL63, SARS-CoV-1, and SARS-CoV-2 (
Li et al., 2003). Additionally, cellular proteases, such as TMPRSS2, cathepsin L, and furin, are important for the cleavage of the viral spike (S) protein of several coronaviruses thereby mediating efficient membrane fusion with host cells (
Simmons et al., 2005). Systematic studies have illuminated virus-host interactions during the later steps of the viral life cycle. For example, proteomics approaches revealed comprehensive interactomes between individual coronavirus proteins and cellular proteins (
Stukalov et al., 2020). Additionally, biotin labeling identified candidate host factors based on their proximity to coronavirus replicase complexes (
V’kovski et al., 2019). While these studies uncovered physical relationships between viral and cellular proteins, they do not provide immediate information about the importance of these host components for viral replication.
An orthogonal strategy is to screen for mutations that render host cells resistant to viral infection using CRISPR-based mutagenesis. These screens identify host factors that are functionally required for viral infection and could be targets for host-directed therapies (
Puschnik et al., 2017). In this study, we have performed a genome-wide CRISPR knockout (KO) screen using SARS-CoV-2 (USA/WA-1 isolate) in human cells. Importantly, we expanded our functional genomics approach to distantly related Coronaviridae members in order to probe for commonalities and differences across the family. This strategy can reveal potential pan-coronavirus host factors and thus illuminate targets for antiviral therapy to combat the current and potential future outbreaks. We conducted comparative CRISPR screens for SARS-CoV-2 and two seasonally circulating common cold coronaviruses, OC43 and 229E. Our results corroborate previously implicated host pathways, uncover new aspects of virus-host interaction, and identify targets for host-directed antiviral treatment.
Results
CRISPR KO Screens Identify Common and Virus-Specific Candidate Host Factors for Coronavirus Infection
Phenotypic selection of virus-resistant cells in a pooled CRISPR KO screen is based on survival and growth differences of mutant cells upon virus infection. We chose Huh7.5.1 hepatoma cells as they were uniquely susceptible to all tested coronaviruses. We readily observed drastic cytopathic effect during OC43 and 229E infection (Figure S1A). Huh7.5.1 also supported SARS-CoV-2 replication but exhibited limited virus-induced cell death (Figures S1B and S1C). To improve the selection conditions for the SARS-CoV-2 CRISPR screen, we overexpressed ACE2 and/or TMPRSS2, which are present at low levels in wild-type (WT) Huh7.5.1 cells (Figure S1D). This led to increased viral uptake of a SARS-CoV-2 S-pseudotyped lentivirus, confirming the important function of ACE2 and TMPRSS2 for SARS-CoV-2 entry (Figure S1E). We ultimately used Huh7.5.1 cells harboring a bicistronic ACE2-IRES-TMPRSS2 construct for the SARS-CoV-2 screen as these cells sustained efficient infection that led to widespread cell death while still allowing the survival of a small number of cells (Figures S1C and S1F). The generated CRISPR KO libraries in Huh7.5.1 and Huh7.5.1-ACE2-IRES-TMPRSS2 cells had virtually complete single-guide RNA (sgRNA) representation prior to the start of the virus challenge but, as expected, were depleted of cells containing sgRNAs against commonly essential fitness genes within 7 days post-library transduction (Figures S1G and S1H) (
Figure S1Optimization of Phenotypic Selection of Coronavirus-Infected Huh7.5.1 Cells and Quality Control Metrics for CRISPR Screens, Related to Figure 1
The three CRISPR screens—for resistance to SARS-CoV-2, 229E, and OC43—identified a compendium of critical host factors across the human genome (Figure 1A; Table S1). The overall performance of the screens was robust as indicated by the enrichment of multiple individual sgRNAs against the top 10 scoring genes from each screen (Figure S1I). Importantly, the known viral entry receptors ranked among the top hits: ACE2 for SARS-CoV-2 and aminopeptidase N (ANPEP) for 229E (Figures 1B and 1C) (
Yeager et al., 1992). OC43, unlike the other coronaviruses, does not have a known proteinaceous receptor but primarily depends on sialic acid or glycosaminoglycans for cell entry (
Ströh and Stehle, 2014); consistent with this fact, multiple heparan sulfate biosynthetic genes (B3GALT6, B3GAT3, B4GALT7, EXT1, EXT2, EXTL3, FAM20B, NDST1, SLC35B2, UGDH, XYLT2) were identified in our OC43 screen (Figures 1D and S2A). Several of these genes were also markedly enriched in the SARS-CoV-2 screen (Figures 1B and S2A), which is consistent with a recent report that SARS-CoV-2 requires both ACE2 and cellular heparan sulfate for efficient infection (
Clausen et al., 2020). Overall, the identification of the expected entry factors validates the phenotypic selection of our host factor screens.
Figure 1Genome-wide Loss-of-Function Screens in Human Cells Identify Host Factors Important for Infection by SARS-CoV-2, 229E, and OC43
Melanie Ott co-led a study with researchers from Gladstone, the Chan Zuckerberg Biohub, UC San Francisco, and Synthego Corporation that points toward ways to treat not only COVID-19, but future coronaviruses that might emerge.
"When a coronavirus—including SARS-CoV-2, which causes COVID-19—infects someone, it hijacks the person’s cells, co-opting their molecular machinery for its own survival and spread. Researchers at Gladstone Institutes and the Chan Zuckerberg Biohub, in collaboration with scientists at UC San Francisco (UCSF) and Synthego Corporation, have identified critical molecular processes in human cells that coronaviruses use to survive.
They report, in a study published in the journal Cell, that targeting these processes with drugs may treat not only COVID-19 infections, but other existing and future coronaviruses.
“What is unique about our study is that we didn’t just look at SARS-CoV-2, but other coronaviruses at the same time,” says one of the leaders of the study, Melanie Ott, MD, PhD, director of the Gladstone Institute of Virology. “This gives us a good idea of drug targets that could broadly suppress many coronaviruses.”
A large family of viruses, coronaviruses include common cold viruses as well as more severe viruses. The SARS-CoV virus that caused a deadly SARS epidemic in 2002 was a coronavirus, as is the MERS virus, which has caused outbreaks in the Middle East.
“There have now been multiple coronavirus outbreaks, so it’s clear this virus family has high pandemic potential,” says Andreas Puschnik, PhD, a principal investigator at the Chan Zuckerberg Biohub and the other leader of the study. “COVID-19 is not the last coronavirus infection we’ll be dealing with.”
Comparing and Contrasting Coronaviruses
Like all viruses, coronaviruses can only grow inside host cells; they rely on the host cell’s molecules to multiply. Because of this, the team of researchers want to target human molecules that the viruses use to survive, rather than components of viruses themselves.
In the new study, they infected human cells with either SARS-CoV-2 or two other coronaviruses that cause common colds—and all three viruses killed the cells. Next, the team of researchers mutated the cells using CRISPR-Cas9 gene-editing technology and studied which mutations made the cells less vulnerable to the coronaviruses.
“We reasoned that the few cells that could survive these infections presumably had mutations in host molecules that the viruses use to infect them or to multiply,” explains Puschnik.
Some results were not surprising. For instance, the human ACE2 receptor is known to be required by SARS-CoV-2 to enter human cells. So, cells with a mutation in the ACE2 gene were no longer infected or killed by SARS-CoV2.
But other findings were less expected. The researchers found that certain genetic mutations prevented all three coronaviruses from successfully infecting and killing the cells. These were mutations in genes known to control the balance of two types of lipid molecules in human cells, namely cholesterol and phosphatidylinositol phosphate (PIP).
Cholesterol is needed for some viruses to enter cells, but it hadn’t been studied in the context of coronaviruses when this study started. Similarly, PIP is known to play a role in forming the small vesicles that viruses often use to travel into and around cells, but it had not been directly linked to SARS-CoV-2 before.
A Pathway toward Therapeutics
To verify the importance of the cholesterol and PIP genes for coronavirus infection, the researchers engineered human cells that lack these genes completely and infected them with the virus. Cells lacking the genes were protected from infection by all three coronaviruses. Similarly, when the team used existing compounds to disrupt the balance of PIP or cholesterol, the cells were less susceptible to infection by any of the viruses.
These results suggest that targeting cholesterol or PIP could be a promising strategy to combat multiple coronaviruses.
“For viruses, the traditional view has been that we design drugs against unique viral targets, and that means it takes time to develop a drug each time there’s a new virus,” says Ott, who is also a professor in the Department of Medicine at UCSF. “If we could develop a few broader antiviral drugs that target host cells’ molecules, that would go a long way toward making us better prepared for future pandemic viruses.”
Not all results were the same between the three studied viruses, however. Some human molecules required for SARS-CoV-2 infection weren’t needed by the two common cold coronaviruses, and vice versa. These findings could help explain what makes SARS-CoV-2 more deadly than the other two viruses.
More work is needed to test the effectiveness of drugs targeting PIP and cholesterol, and whether they can effectively stop viral growth without causing dangerous side effects. The team would also like to repeat the screens using other coronaviruses—including the first SARS-CoV and MERS viruses—to determine just how universal the new targets they pinpointed are.
Ott and Puschnik agree that the current study was made possible by researchers from many labs coming together without hesitation. Puschnik has expertise in studying viral host factors, but didn’t have access to a Biosafety Level 3 (BSL-3) lab required to work with SARS-CoV-2. Ott was spearheading Gladstone’s effort to open such a lab earlier this year and offered to collaborate. Scientists at Synthego provided the engineered cells needed to study the viruses, and Gladstone Senior Investigator Nevan Krogan, PhD, helped analyze the results of the CRISPR-Cas9 screen.
“Everybody was completely willing to roll up their sleeves, pool resources, and work together to help contribute to better understanding COVID-19,” says Puschnik."
"It probably indicates that we’ve evolved defense mechanisms in the airway to not fall completely prey to coronaviruses. Once the virus gains access, it can distribute and disseminate and go into other organs pretty easily, and then we have big problems. The airway epithelium is the first layer of defense. So, in my mind it speaks to the fact that coronaviruses have been around for a while.
What will you learn from manipulating genes with CRISPR? We can figure out which host proteins the virus really needs, because when we get rid of them with CRISPR, the virus can’t replicate. We can also find what we call restriction factors – host proteins that stop the virus from replicating. When we get rid of them, the virus replicates much more. Finding proteins in both of these groups can help us develop new treatments for COVID-19.
WHAT WOULD BE YOUR IDEAL OUTCOME FROM THE PROJECT?
The ideal outcome would be to find a drug target that is effective against SARS-CoV-2 but also other coronaviruses. The advantage of targeting host factors is that some are likely shared between multiple viruses. Finding those host factors can help in developing pan-antivirals which hopefully will be ready to tackle the next pandemic virus on the horizon."
According to independent analyses by NASA and the National Oceanic and Atmospheric Administration (NOAA), Earth’s surface temperatures in 2019 were the second warmest since
modern recordkeeping began in 1880. Globally, 2019 temperatures were second only to those
in 2016 and continued the planet’s long-term warming trend. The past five years have been the warmest of the past 140 years.
In 2019, global temperatures were 0.98 degrees Celsius (1.8 degrees Fahrenheit) warmer than the 1951 to 1980 mean, according to scientists at NASA’s
Goddard Institute for Space Studies. The map above depicts global temperature anomalies in 2019. It does not show absolute temperatures; instead, it shows how much warmer or cooler each region of Earth was compared to that baseline average.
“The decade that just ended is clearly the warmest decade on record,” said GISS director Gavin Schmidt. “Every decade since the 1960s clearly has been warmer than the one before.”
The animated plot below shows yearly temperature anomalies from 1880 to 2019 with respect to the 1981-2000 mean, as recorded by NASA, NOAA, the Berkeley Earthresearch group, the Met Office Hadley Centre (UK), and the Cowtan and Way analysis. Though there are minor variations from year to year, all five temperature records show peaks and valleys in sync with each other. All show rapid warming in. the past few decades, and all show that the past decade has been the warmest.
Since the 1880s, the average global surface temperature has risen more than 1 degree Celsius (2 degrees Fahrenheit) above the late 19th century. For reference, the last Ice Age was about 5.5 degrees Celsius (10 degrees Fahrenheit) colder than pre-industrial temperatures.
Using climate models and statistical analysis of global temperature data, scientists have concluded that this increase mostly has been driven by increased emissions into the atmosphere of carbon dioxide and other greenhouse gases produced by human activities.
“We crossed over into more than 2 degrees Fahrenheit warming territory in 2015 and we are unlikely to go back,” Schmidt said. “This shows that what’s happening is persistent, not a fluke due to some weather phenomenon. We know that the long-term trends are being driven by the increasing levels of greenhouse gases in the atmosphere.”
Because weather station locations and measurement practices change over time, the interpretation of specific year-to-year global mean temperature differences has some uncertainties. Taking this into account, NASA estimates that the global mean
change in 2019 is accurate to within 0.1 degrees Fahrenheit, with a 95 percent certainty level.
Weather dynamics often affect regional temperatures, so not every region on Earth experienced similar amounts of warming. NOAA found the 2019 annual mean temperature for the contiguous 48 United States was the 34th warmest on record, giving it a “warmer than average” classification.
The Arctic has warmed three times faster than the rest of the planet since 1970. Rising temperatures in the atmosphere and ocean are contributing to the continued mass loss from Greenland and Antarctica and to increases in some extreme events, such as heat waves, wildfires, and intense precipitation.
NASA’s temperature analyses incorporate surface temperature measurements from more than 20,000 weather stations, ship- and buoy-based observations of sea surface temperatures, and temperature measurements from Antarctic research stations. These in situ measurements are analyzed using an algorithm that considers the varied spacing of temperature stations around the globe and urban.
heat island effects that could skew the conclusions. These calculations produce the global average temperature deviations from the baseline period of 1951 to 1980.
NOAA scientists used much of the same raw temperature data, but with a different interpolation into the Earth’s polar and other data-poor regions. The NOAA analysis found 2019 global temperatures were 0.95 degrees Celsius...
(1.7 degrees Fahrenheit) above the 20th century average.
NASA’s full 2019 surface temperature data set and the complete methodology used for the temperature calculation and its uncertainties are available here.
NASA Earth Observatory images by Joshua Stevens, using data courtesy of Gavin Schmidt/NASA and the Goddard Institute for Space Studies. Story by Maria-Jose Vinas Garcia, NASA Earth Science News Team.
News and Blogs
Provincial Leadership on a National Pharmacare Program
Broadbent Institute | Institut Broadbent / February 02, 2021
February 2, 2021
The Honourable John Horgan, M.L.A., Premier of British Columbia
The Honourable Adrian Dix, M.L.A., Minister of Health
Re: Provincial Leadership on National Pharmacare Program
Dear Premier Horgan and Minister Dix,
Canadians cherish their Medicare system. This support crosses all geographic, demographic and political divides. There is a reason that Tommy Douglas was famously voted the “Greatest Canadian”: and that reason is his role – and that of the Co-operative Commonwealth Federation (CCF) – in bringing single-payer public health insurance to this country.
Since the introduction of the 1947 Saskatchewan Hospitalization Act, the CCF/NDP have – as a core mandate – advanced the vision of Medicare as a right of citizenship for Canadians.
We are writing you to ask you to once again fulfill this historic mission through ensuring the government of British Columbia becomes a leading voice in the national effort to achieve universal, public Pharmacare.
Tommy Douglas’s vision for Medicare wasn’t supposed to end at the hospital door. As you know, Canada is the only nation with a single-payer healthcare system that does not include the cost of drugs in that system. Canadians, by an overwhelming margin, believe this flaw in Medicare needs to be fixed.
In a recent poll by the Angus Reid Institute conducted in partnership with UBC’s School ofPopulation and Public Health; St. Michael’s Hospital and University of Toronto; the CarletonUniversity Faculty of Public Affairs and School of Public Policy and Administration; andWomen’s College Hospital, Toronto, nearly 9 in 10 Canadians support a national Pharmacareprogram.
This near unanimity is at least partly explained by the stresses of the COVID-19 pandemic. Inthe same poll, nearly one quarter of Canadians reported that they have recently decided not tofill a prescription or not to renew one due to cost or taken measures to extend it because theycould not afford to keep the recommended dosage schedule.
In the September 23, 2020 Speech from the Throne, the federal government again committed toa universal national Pharmacare program and to “accelerate steps to achieve this system.”
This federal commitment was affirmed again earlier this year in the new mandate letter to the federal minister of health, issued on January 15, which asked that the federal minister work “with provinces and territories that are willing to move forward without delay, [to] accelerate steps to achieve a national, universal pharmacare program”, recognizing that the work needs to be accelerated given “COVID-19 has intensified the health inequities and barriers to care across the country”.
It is imperative that this commitment be made real through a line item in the upcoming federal budget and in keeping with the recommendations from the final report of the Advisory Council on the Implementation of National Pharmacare.
As per the timeline in the Advisory Council’s final report, a national formulary of essential medicines should come into force by January 1, 2022. Considering the growing and urgent need for universal Pharmacare – with hundreds of thousands of people having lost access to employer-sponsored drug plans in recent months – we are calling for this process to be expedited, so that essential medicines can be made available on a universal basis by July 1, 2021.
In the midst of COVID-19, we cannot delay access to essential medicines any further. Hospitals are overwhelmed with patients across the country, and the risk of airborne transmission of the virus has been firmly established. To avoid unnecessary hospital visits that result from a lack of access to prescribed medications, we urgently need universal access to a list of essential medicines.
We have called upon the federal government to dedicate $3.5 billion toward universal coverage for a list of essential medicines – as recommended by the Advisory Council’s final report – in the 2021 Federal Budget. We have also called upon the federal government to usher in this program by July 1 to speed up access for those in need.
On July 1, 1958, the Hospital Insurance and Diagnostic Services Act came into force, and on that day in 1968, the Medical Care Act came into force. Having a list of essential medicines accessible to all people in Canada by July 1, 2021, would begin the fulfillment of an essential yet missing piece of Medicare. And it would do so on the most fitting of days – marking 153 years since Confederation – for our country’s most cherished achievement.
We recognize that Pharmacare cannot move ahead without the participation of the provinces and territories. We are encouraged by the federal government’s Speech from the Throne commitment to work “…with provinces and territories willing to move forward without delay”. We are also pleased with your government’s recent platform commitment to universal pharmacare and the stipulation in Minister Dix’s mandate letter that he continue to fight to make sure the federal government remains focused on a national pharmacare program so you can bring down the cost of pharmaceuticals to make life more affordable for all British Columbians.
At this critical moment, Canadians need British Columbia to lead. Your government can play a key role in the creation of this new social program for all Canadians. Your voice, your actions, will be central to the debate in the weeks and months ahead.
We look forward to working with you to accelerate the implementation of a national, universal, public and single-payer Pharmacare program, and to the completion of Tommy Douglas’s Medicare vision.
Sincerely,
Rick Smith Executive Director, Broadbent Institute
Laird Cronk President, BC Federation of Labour
Anita Huberman CEO, Surrey Board of Trade
Jeff Sommers Director, Health and Policy Systems, BC & Yukon Heart and Stroke Foundation
Mark Hancock National President, Canadian Union of Public Employees
Steve Morgan, PhD Professor of health policy at UBC and Founder of Pharmacare 2020
Pauline Worsfold, RN Chair, Canadian Health Coalition
Marie Clarke Walker Secretary-Treasurer, Canadian Labour Congress
Danyaal Raza Chair, Canadian Doctors for Medicare
Christina Warner and Ravi Joshi Co-Executive Directors, Council of Canadians
Josh Bizjak Executive Director, Douglas-Coldwell Foundation
Linda Silas President, Canadian Federation of Nurses Unions
Larry Brown President, National Union of Public and General Employees
HOW FAR ALONG ARE YOU AND YOUR TEAM IN CREATING "TIPS" AS A VIRAL "HIJACK" THERAPY?
WHEN DO YOU EXPECT THERAPEUTIC INTERFERING PARTICLES OR "TIPS" TO BECOME A MAINSTREAM THERAPY AGAINST COVID-19?
WHICH LARGE COMPANIES ARE INTERESTED IN PRODUCING "TIPS"?
Leor Weinberger, PhD, senior investigator and virologist has pioneered an innovative approach to fighting the spread of viral pathogens. His approach is called therapeutic interfering particles or (TIPs), which could be an alternative to a vaccine. He also directs the Center for Cell Circuitry.
"Prevention
A Gladstone team is investigating the potential of an innovative alternative to a vaccine. Therapeutic interfering particles (TIPs) could turn the tables on the virus by hijacking its machinery to transform virus-infected cells into factories that produce more therapeutic particles than virus, slowing its spread.
Dr. Leor Weinberger has developed a new approach to fight the spread of viruses. It is called therapeutic interfering particles (TIPs) and could be an alternative to a vaccine. TIPs are defective virus fragments that mimic the virus but are not able to replicate. They combat the virus by hijacking the cell machinery to transform virus-infected cells into factories that produce TIPS, amplifying the effect of TIPs in stopping the spread of virus. TIPs targeting COVID-19 would transmit along the same paths as the virus itself, and thus provide protection to even the most vulnerable populations.
Treatment
Gladstone researchers mapped interactions between human host cell proteins and the virus, and are now using this information to identify therapeutic targets. Others are screening libraries of FDA-approved drugs and testing their effects on the virus in human lung “organoids” and human heart cells. Additional projects include investigating how the virus affects the brain, leading to cerebrovascular complications and stroke, and studying ways to rejuvenate the immune system to improve its ability to fight infection.
Diagnostics
Gladstone scientists are collaborating to develop a CRISPR-based method to rapidly measure COVID-19 RNA. By combining the technique with smartphone technology, they aim to develop a diagnostic that could deliver rapid results and be widely deployed even far from traditional labs, such as in airports and other ports of entry, and in remote communities throughout the world. Another team is applying machine learning to discover biomarkers that will predict which patients are most likely to experience severe disease, and which may have an asymptomatic course."
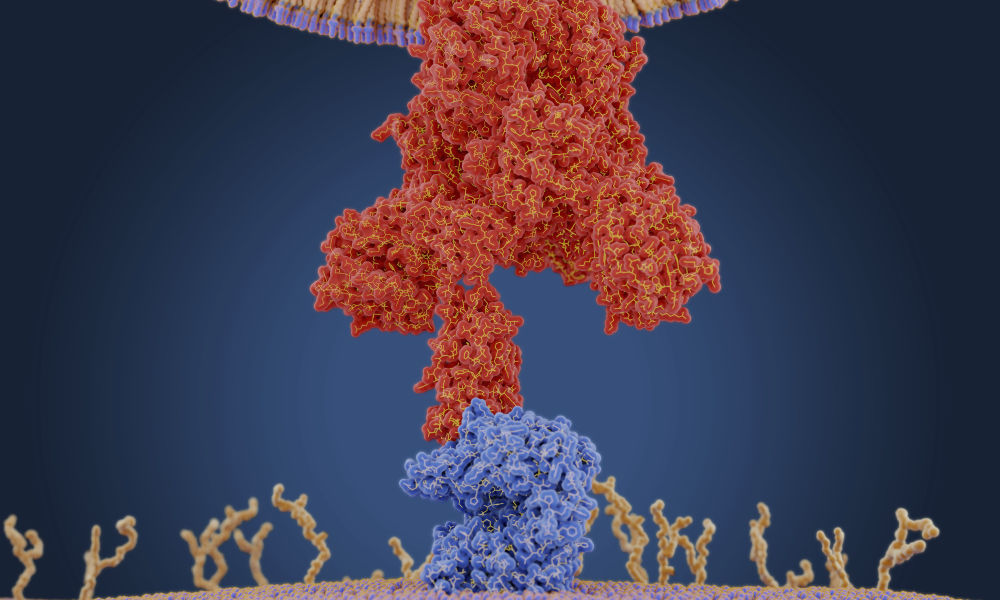
A coronavirus uses a protein on its membrane—shown here in red in a molecular model—to bind to a receptor—shown in blue—on a human cell to enter the cell. Once inside, the virus uses the cells' machinery to make more copies of itself. (Juan Gaertner / Science Source)
How does coronavirus infect humans?
In mammals, such as humans, DNA contains genetic instructions that are transcribed—or copied—into RNA. While DNA remains in the cell’s nucleus, RNA carries the copies of genetic information to the rest of the cell by way of various combinations of amino acids, which it delivers to ribosomes. The ribosomes link the amino acids together to form proteins that then carry out functions within the human body.
Many diseases occur when these gene expressions go awry.
What does RNA stand for?
RNA stands for ribonucleic acid.
What is RNA?
RNA delivers the genetic instructions contained in DNA to the rest of the cell.
COVID-19, short for “coronavirus disease 2019,” is caused by the novel coronavirus SARS-CoV-2. Like many other viruses, SARS-CoV-2 is an RNA virus. This means that, unlike in humans and other mammals, the genetic material for SARS-CoV-2 is encoded in ribonucleic acid. The viral RNA is sneaky: its features cause the protein synthesis machinery of our cells to mistake it for RNA produced by our own DNA.
While SARS-CoV-2 is a new coronavirus, “it likely replicates and functions similar to related coronaviruses that infect animals and humans,” says Douglas Anderson, an assistant professor of medicine in the Aab Cardiovascular Research Institute and a member of the Center for RNA Biology, who studies how RNA mutations can give rise to human disease.
A graphic created by the New York Times illustrates how the coronavirus that causes COVID-19 enters the body through the nose, mouth, or eyes and attaches to our cells. Once the virus is inside our cells, it releases its ribonucleic acid. Our hijacked cells serve as virus factories, reading the virus’s ribonucleic acid and making long viral proteins to compromise the immune system. The virus assembles new copies of itself and spreads to more parts of the body and—by way of saliva, sweat, and other bodily fluids—to other humans.
“Once the virus is in our cells, the entire process of infection and re-infection depends on the viral RNA,” Maquat says.
“Understanding RNA structure and function helps us understand how to throw a therapeutic wrench into what the COVID-19 RNA does—make new virus that can infect more of our cells and also the cells of other human beings,” says Lynne Maquat, professor of biochemistry and biophysics at the University of Rochester Medical Center and the director of Rochester’s Center for RNA Biology.
Saturday, January 30, 2021
Dear CANADIAN GOVERNMENT.
Money money money makes the world go down...the world go down...the world go down. Your political policies are defensive and unimaginative and stifled by protocols created during past years of POLITICAL indoctrination. I am not an industrial polluting CAPITALIST nor a dangerous dominating COMMUNIST nor a middle of the road SOCIALIST. I am a HUMAN BEING! A HOMO SAPIEN NATURALIST AND AN ECOLOGIST and I am forced to survive under Americanized federal Imperialism mixed with corporate business Fascism. I am constantly bombarded by COMMERCIAL ADVERTISING attempting to literally indoctrinate me into becoming a subservient CONSUMER. MY OWN CANADIAN GOVERNMENT attempts to sell dangerous polluting Oil to the World in order to maintain an ECONOMY based on AN IMPERIAL SOCIAL ORDER. ON TOP OF OUR POLITICAL SOCIAL ORDER SITS HER MAJESTY THE QUEEN, WHO believes an invisible DEITY knows all and sees all and gives her (THE QUEEN) absolute power over her Empire. She believes her dominance is a God given right. The fact that Life evolved and created CLEVER MEN who then created dozens of Gods to pacify AND DOMINATE humanity continues to escape the intelligence of millions of brainwashed people. The fact that industrial pollution creates a friendly environment for DANGEROUS pandemic causing viruses, also seems to be outside the moral and mental capacity of millions of people! Specifically, corrupt money and power hungry BUSINESS IMPERIAL imitators WHO ARE are the most dangerous people on Earth! WHY? Because they want to maintain the status-quo by selling Oil based products to the world. Thanks for reading... signed: Grumpy old man. P.S. I dare you to throw these concepts into your political agenda.








31626-3&id=fx1.jpg){kind=link}
31626-3&id=figs1.jpg){kind=link}
31626-3&id=gr1.jpg){kind=link}